If you’re reading this at 2am, the most useful thing this article can do is not add to your to-do list. Every May, Better Sleep Month brings a wave of 31-day plans aimed at families with babies. And across more than 68,000 families in our research (68,366 to be exact), the assumption that your baby’s sleep is broken is wrong more often than it’s right.
Most of what parents call broken baby sleep falls inside the normal developmental range for that age in our 68,000-family dataset.
Better Sleep Month was created in 1985 as a public-health awareness initiative, not as a 31-day household challenge – the challenge framing is industry, not science.
Permission to wait two weeks before changing anything is a valid Better Sleep Month plan.
Three small moves outperform most 31-day programs: notice for a few days, change one environment thing, protect your own bedtime once.
Persistent breathing changes during sleep, total sleep below the AASM range across multiple weeks, or missed milestones warrant a pediatrician, not an app.
Every May, Better Sleep Month shows up in newsletters, apps, and parenting feeds with a pretty consistent message: your family’s sleep is broken, and here is the program to fix it. The data we work with at Betteroo, and the families we work with, keep telling a different story.
What Better Sleep Month Was Supposed to Be
Better Sleep Month was created by the Better Sleep Council in 1985 as a public-health awareness initiative. It was meant to remind people that sleep matters. It was not meant to launch an industry of 31-day household challenges.
That’s what it has become for parents of babies. Open any sleep app or newsletter this month and the implicit message is the same: your family’s sleep is broken, and here’s the program to fix it.
We work with the data and the families, and we keep finding the same thing. Most of what feels broken at 3am is your child’s nervous system doing exactly what it is supposed to do at that age. That’s not nothing – it’s exhausting. But it’s also not a problem you’ve failed to solve. (If you’ve been getting your sleep advice from AI Overviews this year, that’s often part of why something feels off – they’re wrong on baby sleep more often than parents realize.)
What 68,000 Families Tell Us About Baby Sleep
In our 2026 family sleep dataset of more than 68,000 families, the majority of parents who described their baby’s sleep as “broken” had data that fell inside the American Academy of Sleep Medicine’s normal range for that age. Frequent night wakings between 3 and 9 months are typical. Wake-ups during the 4-month and 8-9 month windows are typical. A baby who needs help to fall back asleep is typical. None of that means it’s easy.
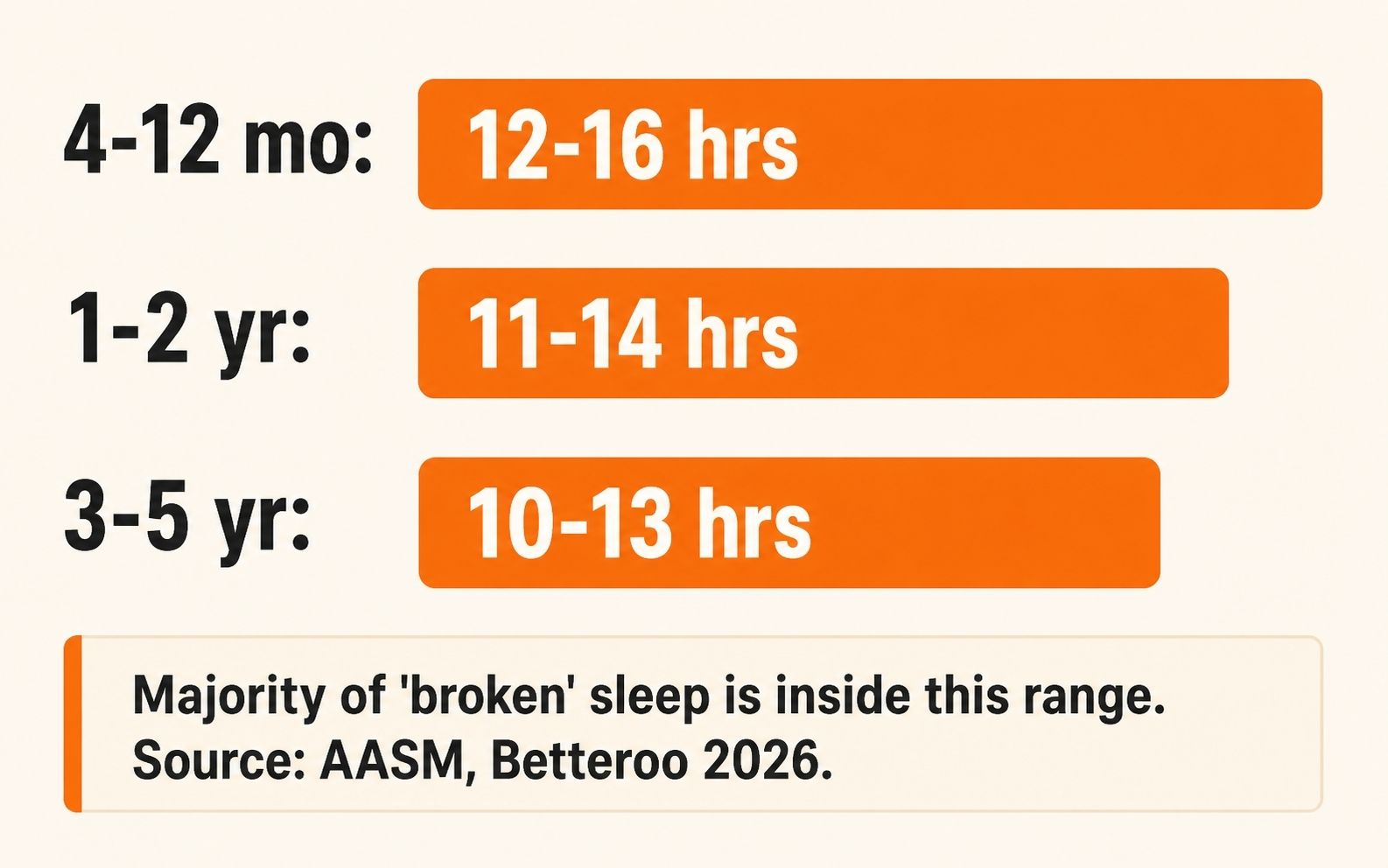
The table below sits this in context. AASM publishes consensus ranges for total sleep across 24 hours by age. If your child is broadly inside the range, has no breathing concerns during sleep, and is meeting milestones, frequent wakings are usually a phase, not a defect.
Age
AASM Total Sleep (24h)
What This Often Looks Like
4-12 months
12-16 hours (incl. naps)
1-3 night wakings; 2-4 naps consolidating to 2
1-2 years
11-14 hours (incl. naps)
1 wake or none most nights; 1-2 naps
3-5 years
10-13 hours (incl. naps)
Mostly through-the-night; nap drops by ~4
If you want to dig into what’s actually normal for your child’s exact age, that piece breaks the year down month by month. The fastest answer for most parents reading this in May is: probably more normal than the internet has been telling you.
“The biggest gift Better Sleep Month could give parents of babies is permission to wait two weeks before changing anything. That’s often how long it takes to see whether the ‘problem’ was actually a phase.”
This is not an attack on every sleep plan. Some of them help. But five recurring errors show up in the prescriptive 31-day content this month, and they’re worth naming.
1. They prescribe before they observe.
Most plans ask you to start fixing on day one. Pediatricians do the opposite – they ask for a week of tracking before recommending changes. The reason is simple: the variable that is keeping your family up is rarely the one you would have guessed from inside the experience.
2. They isolate the baby from the household.
Research on family sleep dynamics finds that household sleep quality tracks with the entire system – the latest adult bedtime, the room sharing setup, the older sibling, the partner schedule. A plan that only changes the baby’s behavior leaves most of the system untouched.
3. They treat normal variation as broken.
This is the big one. The 4-month sleep regression is not a regression in the medical sense – it is the moment a baby’s sleep architecture matures. It looks like things are falling apart because the brain is reorganising. A plan that treats this as a defect to defeat will frustrate you. Recognising it as a developmental phase will not make it less tiring, but it changes the question from “what am I doing wrong” to “what does my baby need right now.”
4. They conflate sleep training with sleep improvement.
Sleep training is one specific tool: teaching independent sleep through structured response. Sleep improvement is the broader change in your family’s sleep system. They are not the same. You can dramatically improve sleep with environment fixes and a baby sleep schedule by age appropriate to your child without ever doing formal training. If you do want a method, common sleep training methods walks through the options. Either is valid. Conflating them is what leads to the “I tried sleep training and it didn’t work” story when what was tried was usually neither full training nor sustained long enough to evaluate.
5. They ignore parent recovery.
If you are sleep-deprived, the case for protecting your own bedtime is not optimization – it is recovery. The version of you that has slept five hours in two stretches is not the same parent as the version of you that slept five hours straight. Most plans treat parent sleep as out of scope. It is the most under-tracked variable we see.
1
What 31-day plans do
Prescribing before observing.
→ What to do instead
Notice for a few days. Don’t commit to changes until you can name the actual pattern.
2
What 31-day plans do
Isolating the baby from the household.
→ What to do instead
Ask which household variable is the loudest, not just which baby behavior.
3
What 31-day plans do
Treating normal variation as broken.
→ What to do instead
Compare to AASM age ranges before assuming the issue is a defect.
4
What 31-day plans do
Conflating sleep training with sleep improvement.
→ What to do instead
Decide if you want a method, or whether environment + schedule changes are enough.
5
What 31-day plans do
Ignoring parent recovery.
→ What to do instead
Treat your own sleep ceiling as a clinical variable, not a luxury.
If reading this is making you wonder where your family actually sits relative to that 68,000-family dataset, that is exactly what the Betteroo quiz was built for.
Wondering where your family sits?
Take the free Betteroo quiz. Five minutes, built from data on 68,000+ families. We will tell you what we see.
If your week has bandwidth for nothing, the only thing that matters is that everyone is safe tonight. Read no further. Come back when there is room.
If there is some room, three small, low-energy moves are worth more than a 31-day program.
Notice for a few days. Not a tracker, not an app, not a spreadsheet – just pay attention to what actually happens at bedtime and overnight without trying to change it. Most parents discover the issue is not what they thought.
Make one environment change. The fastest wins are always environmental: a darker room, a steadier sound, a cooler temperature. If you already have a steady sound machine running but it cycles or has lights, fixing that one thing is often more than you would get from any 31-day plan.
Protect your own bedtime once this week. Not every night. Once. Treat it as care, not discipline. The data on family sleep ecology is clear that your recovery is part of the system.
Doing none of this is also a valid plan. The goal isn’t Better Sleep Month. The goal is your family.
When to Move From Noticing to a Plan
Reach out to your pediatrician, not just your sleep app, if any of the following are happening:
Persistent breathing changes during sleep – snoring with pauses, unusually heavy breathing, or anything that feels off.
Total sleep consistently below the AASM range for your child’s age across multiple weeks (not single bad nights).
Missed developmental milestones alongside the sleep concern.
A significant feeding change that coincides with the sleep change.
Sudden new behaviors during sleep that don’t soothe with normal interventions.
Outside of those, what you are experiencing is most likely typical. Tiring, but typical. That distinction is the one Better Sleep Month is supposed to deliver.
Frequently asked questions
Is my baby’s sleep normal?+
Across more than 68,000 families in our 2026 dataset, the majority of self-described “broken” baby sleep falls inside the AASM-recommended sleep range for that age. If your child is broadly inside the range, has no breathing concerns, and is meeting milestones, frequent wakings are usually a phase, not a defect.
What is Better Sleep Month?+
Better Sleep Month is a public-health awareness initiative created by the Better Sleep Council in 1985 and observed every May. It was designed to raise awareness, not to launch 31-day household challenges. The challenge framing came later from the consumer sleep industry.
Do 31-day sleep resets actually work?+
Some structured plans help some families. The bigger problem is that most resets prescribe before observing, treat normal developmental variation as broken, and ignore parent recovery. For many families, the most useful intervention is permission to wait two weeks before changing anything.
How do I tell whether it is a phase or a real problem?+
Compare to AASM total-sleep ranges for your child’s age. Watch for breathing concerns during sleep, missed milestones, or feeding changes that coincide with the sleep change. Single bad nights and developmental wake-ups are usually phases. The clinical signals listed above are when a pediatrician matters more than an app.
Should I sleep train during Better Sleep Month?+
If your environment, schedule, and a few days of noticing have not improved things and you still want a structured method, sleep training is a reasonable next step. There is no calendar reason to start in May specifically. The right time is when your family is ready and any acute illness or travel is past.
What about my own sleep?+
Research on family sleep dynamics, going back to foundational work by Meltzer and Mindell, finds household sleep tracks closely with parental sleep and stress, not just the baby’s bedtime. Protecting your own sleep ceiling once a week is recovery, not optimization. It is one of the most useful and most under-tracked moves in family sleep.
Key takeaway
If your child is broadly inside the AASM age-normal sleep range, has no breathing concerns, and is meeting milestones, frequent night wakings during the first 18 months are usually a phase, not a problem – and the most useful Better Sleep Month move for many families is permission to wait, not a 31-day plan.
Permission to wait, with a way to know if waiting is the wrong call.
See where your family sits relative to 68,000 others. Five minutes. No 31-day plan attached.
American Academy of Pediatrics Task Force on Sudden Infant Death Syndrome. (2022). Sleep-Related Infant Deaths: Updated 2022 Recommendations for Reducing Infant Deaths in the Sleep Environment. Pediatrics, 150(1).https://pubmed.ncbi.nlm.nih.gov/35726558/
Paruthi, S., Brooks, L. J., D’Ambrosio, C., et al. (2016). Recommended Amount of Sleep for Pediatric Populations: A Consensus Statement of the American Academy of Sleep Medicine. Journal of Clinical Sleep Medicine, 12(6), 785-786.https://pubmed.ncbi.nlm.nih.gov/27250809/
Meltzer, L. J., & Mindell, J. A. (2007). Relationship between child sleep disturbances and maternal sleep, mood, and parenting stress: a pilot study. Journal of Family Psychology, 21(1), 67-73.https://pubmed.ncbi.nlm.nih.gov/17371111/